Endometriosis is a chronic gynecological condition affecting roughly 10% of reproductive-age women and girls worldwide, translating to nearly 190 million individuals1. The disease develops when tissue resembling the uterine lining grows outside the uterus. Although this tissue responds to hormonal cycles in the same way as normal endometrium, it lacks a pathway to exit the body. As a result, inflammation, irritation, and progressive internal damage occur.
Often described as a “modern epidemic,” endometriosis remains one of the most misdiagnosed conditions in medicine2. Symptoms are frequently normalized or mistaken for routine menstrual discomfort. A deeper understanding of its biological mechanisms is essential to reduce years of unnecessary suffering and delayed care.
Systemic impact and biological drivers
Beyond its gynecological origins, endometriosis behaves as a systemic disorder that involves multiple biological pathways. The disease reflects complex interactions between immune dysfunction, inflammatory signaling, hormonal imbalance, and aberrant cellular migration3-6. Genetic predisposition significantly influences susceptibility, which explains why the condition often clusters within families. Environmental toxins and endocrine disruptors can further amplify lesion growth and persistence7, 8.
Without timely intervention, chronic inflammation may gradually lead to fibrosis, organ distortion, and long-term reproductive complications9-11. Recent advances in imaging physics and materials science are now allowing researchers to investigate the disease at cellular and biomechanical levels. These technologies are reshaping how clinicians conceptualize and manage endometriosis.
Pathophysiology and the mechanics of cellular migration
Understanding how endometrial-like cells establish themselves outside the uterus is central to explaining the progression of endometriosis. Several biological mechanisms contribute to the survival and expansion of these misplaced tissues.
Ectopic implantation and immune failure
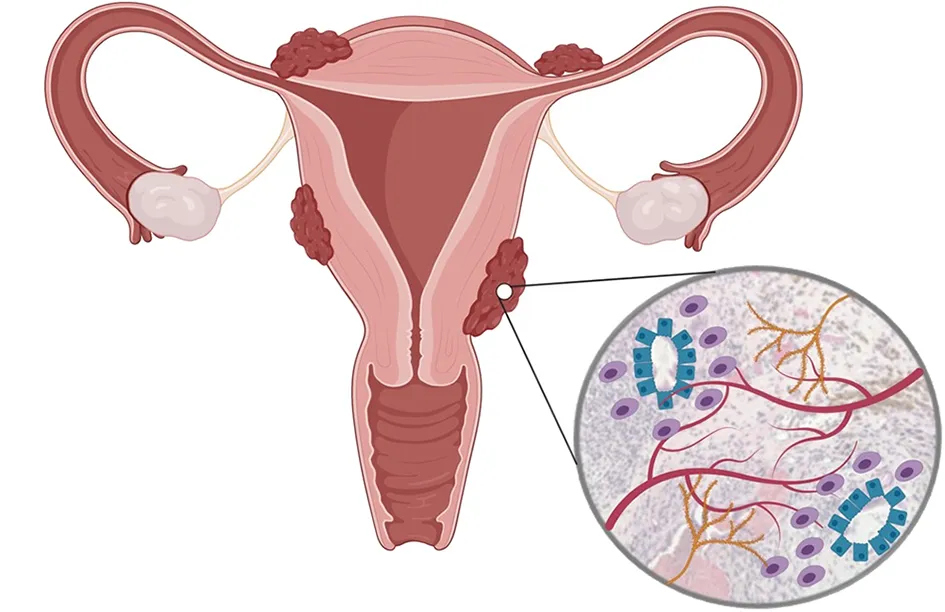
The defining feature of endometriosis is the presence of endometrial-like implants outside the uterus1. These lesions most commonly develop on the ovaries, fallopian tubes, and pelvic peritoneum, although distant sites such as the lungs have occasionally been reported. Retrograde menstruation, in which menstrual blood flows backward into the pelvic cavity, is considered an important contributing factor1. However, this phenomenon alone cannot explain why only certain individuals develop persistent lesions.
Current evidence suggests that a failure of immune surveillance plays a central role12. In healthy systems, immune cells identify and remove misplaced endometrial cells. In endometriosis, this clearance mechanism appears impaired. As a result, the ectopic cells survive, attach, and proliferate. They stimulate angiogenesis and develop their own blood supply, which allows them to respond to estrogen signals in the same way as uterine tissue13. Persistent inflammation then gradually damages surrounding organs and connective tissue1.
Core cellular mechanisms
Once ectopic cells evade immune clearance, several cellular processes allow them to establish stable lesions. The implants adhere to the peritoneal surface using specialized adhesion molecules that function like biological glue14. After attachment, the cells begin producing estrogen locally, which creates a self-sustaining hormonal environment that promotes continued growth.
Nerve fibers gradually infiltrate these lesions, which helps explain the severity and persistence of pain. Over time, ongoing inflammation stimulates adhesion formation that can bind pelvic organs together. This process distorts normal anatomy and contributes to chronic pelvic dysfunction1.
Hydrogels and the physics of tissue modeling
In recent years, materials science has become a valuable tool for studying endometriosis. Researchers are developing synthetic hydrogels that mimic the physical properties of pelvic and endometrial tissues15. These biomimetic scaffolds allow scientists to observe how endometrial cells migrate, attach, and invade surrounding structures under carefully controlled conditions.
By adjusting the stiffness and composition of these hydrogels, researchers can simulate different tissue environments found in the human body. This approach provides important insight into how mechanical forces influence disease progression. It also enables safer testing of drugs designed to block cell adhesion or invasion before they enter clinical trials.
Clinical presentation and daily life impact
Although the biological mechanisms of endometriosis are increasingly understood, the disease is most visible through its impact on everyday life. Symptoms can vary widely, which often complicates early recognition.
Symptom diversity and diagnostic delay
Endometriosis presents with a wide spectrum of symptoms that often overlap with gastrointestinal or urological disorders16, 17. This overlap contributes to the well-documented diagnostic delay, which averages six to ten years and may extend even longer in some regions. For many patients, pain is not limited to menstruation but gradually becomes a persistent feature of daily life.
Recognizing the variability of symptoms is essential for earlier diagnosis. Timely identification allows better symptom control, preserves fertility, and reduces psychological distress associated with prolonged uncertainty.
Reproductive and systemic manifestations
Painful menstruation in endometriosis is often far more severe than typical menstrual cramps, reflecting inflammatory processes rather than normal uterine contractions18. Chronic pelvic pain may persist throughout the month, disrupting work, education, and social relationships19, 20. Pain during or after intercourse is also common and may strain emotional intimacy.
Fertility challenges affect a substantial proportion of patients and frequently lead to the first clinical evaluation21. When lesions involve the bowel or bladder, individuals may experience painful defecation, urinary urgency, or cyclical gastrointestinal symptoms22.
These physical burdens often extend beyond the reproductive system. Persistent pain can disrupt sleep, contribute to fatigue, and impair cognitive clarity23, 24. Systemic inflammation may also influence mood regulation and stress responses. Many individuals report abdominal bloating, often called “endo-belly,” alongside feelings of frustration and bodily betrayal25. When symptoms are dismissed or minimized, psychological distress may intensify and delay care-seeking behavior.
Diagnostic breakthroughs and imaging physics
Given the complexity of symptoms, accurate diagnosis remains one of the greatest challenges in endometriosis care. Fortunately, advances in imaging science are beginning to transform this process.
Moving beyond invasive diagnosis
Laparoscopic surgery has long functioned as the diagnostic benchmark in the clinical assessment of endometriosis26. While effective, the invasive nature of this procedure limits its usefulness for early detection. As such, researchers have increasingly focused on non-invasive diagnostic tools.
Advances in imaging physics are now making earlier identification possible. High-resolution MRI protocols can detect deep infiltrating lesions that previously went unnoticed27. At the same time, improvements in transvaginal ultrasound technology have enhanced the visualization of bowel and pelvic nodules28. Preoperative imaging maps now help surgeons locate lesions with greater precision, which reduces operative time and tissue trauma29.
Emerging biomarkers and AI integration
Alongside imaging advances, scientists are exploring biological markers that could enable simple diagnostic tests. Research into blood and saliva biomarkers, including microRNA signatures and circulating DNA methylation patterns, is progressing rapidly30, 31. These tools aim to provide accessible and non-invasive methods for detecting the disease.
Artificial intelligence is also beginning to assist diagnostic interpretation32. Machine-learning algorithms can analyze imaging patterns and help distinguish endometriosis from benign cysts or other pelvic disorders33. Consistent monitoring through imaging and clinical evaluation allows clinicians to track disease progression and treatment response more accurately. Early identification of deep or ureter-involving lesions may prevent irreversible organ damage and improve fertility outcomes.
Therapeutic strategies and future directions
Although diagnosis has historically been delayed, treatment strategies for endometriosis continue to evolve. Current management focuses on symptom control, fertility preservation, and improving quality of life.
Current management approaches
Hormonal therapies remain common first-line interventions because they suppress estrogen activity and slow lesion growth1. Oral contraceptives and GnRH agonists induce a temporary hypoestrogenic state that reduces cyclical bleeding and inflammation34, 35. These treatments often provide meaningful symptom relief, although they do not eliminate the underlying ectopic tissue.
Because the disease behaves differently in each individual, treatment plans often combine hormonal management with lifestyle adjustments and supportive therapies36.
Surgical and materials-based innovations
When symptoms remain severe or fertility is threatened, surgical excision becomes an important option. Laparoscopic procedures aim to remove lesions while preserving surrounding healthy tissue37. Robotic-assisted techniques allow surgeons to operate with greater precision in anatomically complex regions such as the deep pelvis.
In addition to surgical refinement, materials science has introduced anti-adhesion barriers that reduce the likelihood of organs sticking together after surgery38. Pelvic floor physical therapy is also gaining recognition as a valuable adjunct treatment because it helps retrain muscles that have become chronically tightened by prolonged pain39.
The future of endometriosis care
The future of endometriosis care is shifting from broad hormonal regulation to targeted intervention. Current research is prioritizing immune-modulating and anti-angiogenic pathways to selectively eliminate lesions by cutting off their nutrient supply, offering a more precise alternative to conventional therapy40.
At the same time, there is growing evidence that managing gut health and the gut microbiome can help lower systemic inflammation throughout the pelvic region. Artificial intelligence is also expected to transform how we approach surgery, using advanced mapping to help clinicians locate and treat even the smallest areas of disease32.
New developments across medicine and technology are paving the way for faster, more personalized care for endometriosis41. For the millions of people affected, this progress promises more than just better treatment; it offers the kind of recognition and reliable relief that has been missing for far too long.